assessing drug harms and drug facts
Drug Policy Alliance - MDMA fact sheet
![]()
Facts About MDMA
1. What is MDMA?
MDMA, often referred to as “ecstasy” or “molly”, is short for 3,4 methylenedioxymethamphetamine, a psychoactive drug derived from safrole oil. MDMA produces effects that resemble both stimulants and psychedelics, as well as its signature effect: a feeling of connectedness. It impacts brain function primarily releasing the neurotransmitter serotonin, and also temporarily inhibits its reuptake. MDMA is usually taken orally, whether in pressed pill form, powder or crystal; or sometimes snorted.
MDMA was originally synthesized in 1912 by the drug company Merck.1 However, its psychoactive effects weren’t widely discovered until 1976 when Alexander Shulgin developed a new synthesis method, tested the drug on himself, and shared it with a few friendly psychotherapists.2 Because of the drug’s effects of increasing empathy and reducing fear, it started to be used in psychotherapy practices in the 1970s and early 80s, as well as recreationally. In 1985 it became classified by the federal government as a Schedule I drug, meaning among the “most dangerous,” along with marijuana, LSD and heroin. Studies have shown, however, that MDMA is among the least harmful drugs (see question 6 for more details). Despite its Schedule I status, MDMA is still commonly used at festivals, concerts and clubs; and research is ongoing into its therapeutic benefits.
2. How will MDMA make me feel?
People who use MDMA describe themselves as feeling euphoric, open, accepting, unafraid, and connected to those around them.3 Typically used in social settings like festivals, concerts and clubs, MDMA’s effects are stimulated by visuals, sounds, smells and touch, leading to heightened sensations and a desire to intensify these feelings by dancing, talking and touching.
A typical dose of 80 - 125 mg lasts three to six hours. Some people experience nausea at the outset, but after about 45 minutes, report feelings of relaxation and clarity. MDMA also causes dilation of the pupils and, often, sensitivity to light, as well as possible jaw- clenching, tooth-grinding, muscle tension, faintness, and chills or sweating.
After the drug wears off, the theory from preclinical studies is that brain levels of serotonin (a chemical responsible for maintaining mood balance) are depleted, which can lead in some cases to sadness, anxiety, depression and sleep problems.4 If they occur, these symptoms arise in the several days that follow. Generally, they abate within a week, though frequency of use and higher doses can slow or stop this process.
3. What’s the difference between molly, ecstasy and MDMA?
MDMA is the official scientific name for this drug. “Molly” and “ecstasy” are both commonly-used slang terms.
However, since MDMA is currently illegal and therefore unregulated, anything sold as “molly” or “ecstasy” could range from being pure MDMA, to being cut with other drugs, to containing no MDMA at all.6 The molly market is one of the most adulterated illicit drug markets, meaning it often is cut with other substances.7 (See this full list of what ecstasy or molly may contain.)
4. How can I tell if my molly or ecstasy contains MDMA?
Since MDMA is currently illegal and therefore not regulated, it is very difficult for an individual user to be 100% certain what’s in any given dose. Drug checking, also known as pill testing or adulterant screening, is a harm reduction service that allows users to get more information about what is in their molly or other drugs. It can be done in several ways. The best way involves a precise, high- level testing method called gas chromatography / mass spectrometry (GC/MS). Individuals can send a sample in to ecstasydata.org for testing and wait 2 to 3 weeks for the lab results to be posted online. These results will list all substances present in the sample with complete accuracy.
There are also personal drug checking kits, which use liquid chemical reagents to help potential users get a better understanding of what’s in their substance. These kits come with a color chart that helps people determine what drug (if any) is mostly present in the substance they’ve tested. Users should also know that these kits, while not considered illegal under federal laws, can be considered drug paraphernalia depending on how a state’s law is written. Nonetheless, we do recommend them as the most accessible and quick screening tool.
5. Can you overdose on MDMA?
“Overdose” refers to taking a higher than appropriate dose of a medicine or drug, which can happen with MDMA, but is extremely rare.8 It is much more likely that a problem would occur as a result of MDMA use with contraindicated medications (such as MAOI anti- depressants), preexisting health conditions, overexertion, or dehydration.9 Given the highly adulterated molly market, it’s also more likely to see an unidentified substance cause problems, rather than MDMA itself.
Hyperthermia – a dangerously high increase in body temperature, or heatstroke – is the most common health problem related to MDMA. Hyperthermic reactions result from physical exertion (such as dancing) in an overheated environment without replenishing fluids, which is why it is strongly recommended that users take breaks and consume fluids such as water or electrolyte-replenishing drinks. In extreme cases, hyperthermia can cause liver, kidney or heart failure, or even death.10 To prevent theseharms, we strongly recommend that festivals offer free water and areas for people to cool off.
Another concern for people who take MDMA is hyponatremia – drinking too much water. This causes the sodium in the blood to dilute to critically low levels, and seems to affect women more than men.11 This is why, when available, juices and electrolyte- replenishing drinks are preferable to water.
6. How risky is MDMA compared to other drugs?
As with all alcohol and other drug use, taking MDMA carries risks, albeit comparatively lower than most other drugs.12
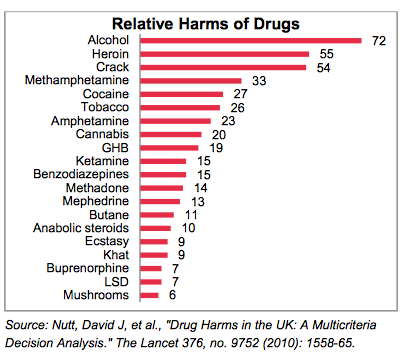
For example, a 2010 study published in the prestigious Lancet journal was conducted to gauge the relative potential harms of drugs to both consumers and to society, and MDMA was found to be among the least risky.13 As you can see in the graph below, overall, alcohol was considered the most harmful drug, with heroin and crack in second and third places. You’ll find MDMA hovering just above the bottom of the scale with a significantly lower rating. Several other researchers have independently reported similar findings.14 It’s clear that a drug’s legal status has little relation to its potential for harm.
7. What are the most common adulterants in what’s sold as “molly” or “ecstasy” (in other words, what chemicals is it commonly cut with)?
Due to being one of the most adulterated drug markets, the impurity of molly in different regions and at different times varies quite a bit – that is, there’s no such thing as the “most common adulterants.” Besides MDMA, “ecstasy” or “molly” may contain varying levels of:
- Psychoactive substances designed to mimic the effects of MDMA like MDA (methylene- dioxyamphetamine a.k.a. “sass”) or “bath salts” (a general term for synthetic cathinones, a class of amphetamine-like stimulants);
- Stimulants like amphetamine, cocaine, caffeine or methamphetamine; or, more rarely Anesthetics such as ketamine (“Special K”) or dextromethorphan (DXM – an ingredient found in over-the-counter cough medicines).
- Anesthetics such as ketamine (“Special K”) or dextromethorphan (DXM – an ingredient found in over-the-counter cough medicines).
All of these can significantly amplify potential harms. The most important thing for harm reduction is to know what you’re getting. According to Ecstasydata.org – an independent laboratory testing program of Erowid Center – among 250 samples they analyzed in 2014 that were sold as molly, 40 samples contained MDMA with adulterants, and nearly half (124) contained no MDMA at all!15
8. What are the long-term health impacts of MDMA?
The long-term health impacts of MDMA are still under investigation, but several studies have found that substances like MDMA have far lower potential to cause harm than legal drugs like alcohol.16
Some researchers suggest that slight brain changes may result from heavy use, such as impacts on memory,17 but the evidence is far from conclusive.18 In fact, MDMA use alone does not appear to cause cognitive differences between people who use it and those who do not.19 Evidence also shows that “[a]dverse effects decrease with... abstinence” (that is, the impacts start reversing themselves once you stop taking the drug).20 The main challenge of determining long-term health effects of MDMA is that people who use it often take other drugs as well, making specific impacts very hard to isolate.21
9. How many people use MDMA?
Among the general population, MDMA use is not very common. According to the 2013 National Survey on Drug Use and Health, only 0.3 percent of people aged 12 and older reported using “ecstasy” in the past month, 1 percent reported using it in the past year, and 6.8 percent reported using at least once in their lifetime.22 The statistics for young people break down like this:
- Among young people ages 12-17, just 0.2 percent reported using MDMA in the past month (compared to 7 percent using marijuana and 11.6 percent using alcohol), and 0.9 percent in the past year (compared to 13.4 percent using marijuana and 24.6 percent using alcohol).23
- Four percent of young adults ages 18-25 reported using MDMA in the past year (compared to 31.6 percent using marijuana and 76.8 percent using alcohol), and just 0.9 percent reported using it in the past month (compared to 19.1 percent using marijuana and 59.6 percent using alcohol). 24
- According to the annual Monitoring the Future survey, approximately one percent of college students and other young adults ages 19-28 reported using MDMA in the past month (compared to 21.6 percent using marijuana and 64.9 percent using alcohol).25
A significant portion of this drug’s use, especially among young people, takes place in nightlife and festival settings. Nearly 80,000 young adults around the world who use drugs were surveyed for the Global Drugs Survey in 2014. Among this sample – over 50 percent of whom reported going “clubbing” at least four times per year – MDMA was in the top five drugs used in the past year. More than 20 percent of U.S. respondents reported using MDMA in the past year.26
10. Can MDMA be used as medicine or therapy?
In short, yes. Before MDMA became popular at festivals, concerts, clubs and raves, it was indeed utilized for therapeutic purposes among mental health practitioners. MDMA-assisted therapy combines traditional psychotherapy with the administration of MDMA.27 Because of MDMA’s unique effect of reducing fear and enhancing interpersonal trust, it can be especially helpful in healing psychological and emotional damage from traumas, helping the terminally ill face death, and other difficult-to-treat psychological conditions.28 MDMA has reportedly been used with over 1,000 human subjects in clinical trials without a single serious adverse event. 29
When the U.S. Drug Enforcement Administration (DEA) sought to completely prohibit MDMA in the 1980s, the medical community protested and the DEA’s own administrative law judge ruled that MDMA should not be placed in Schedule I. However, the DEA ignored this ruling and medical research was shut down for almost two decades. Over the past decade, however, there has been a resurgence in research evaluating MDMA’s therapeutic benefits, especially regarding treatment of post-traumatic stress disorder (PTSD). A seminal study published in 2011 found that patients who received MDMA-assisted psychotherapy reported substantial reductions in the severity of their PTSD symptoms.30 These findings have been replicated by other studies, and additional research is underway in the U.S., Canada, and Israel and soon to begin in the U.K. and Australia.31 , 32
-
1 European Monitoring Centre on Drugs and Drugs Addiction, "Methylenedioxymethamphetamine (MDMA or 'Ecstasy') drug profile," http://www.emcdda.europa.eu/publications/drug- profiles/mdma.
2 “Surfing the Rave: Ecstasy Interview with Dr. Alexander Shulgin,” http://www.mdma.net/alexander-shulgin/mdma.html.
3 RL Carhart-Harris et al., "The effect of acutely administered MDMA on subjective and BOLD-fMRI responses to favourite and worst autobiographical memories," International Journal of Neuropsychopharmacology 17, no. 4 (2014); G. Bedi, D. Hyman, and H. de Wit, "Is ecstasy an "empathogen"? Effects of +/-3,4-methylenedioxymethamphetamine on prosocial feelings and identification of emotional states in others," Biol Psychiatry 68, no. 12 (2010): 1134-40; C. M. Hysek, G. Domes, and M. E. Liechti, "MDMA enhances "mind reading" of positive emotions and impairs "mind reading" of negative emotions," Psychopharmacology (Berl) 222, no. 2 (2012); C. M. Hysek et al., "MDMA enhances emotional empathy and prosocial behavior," Soc Cogn Affect Neurosci 9, no. 11 (2014); M. Kirkpatrick et al., "Prosocial effects of MDMA: A measure of generosity," J Psychopharmacol (2015); M. G. Kirkpatrick and H. de Wit, "MDMA: a social drug in a social context," Psychopharmacology (Berl) 232, no. 6 (2015); M. C. Wardle and H. de Wit, "MDMA alters emotional processing and facilitates positive social interaction," Psychopharmacology (Berl) 231, no. 21 (2014).
4 National Institute on Drug Abuse, “What does MDMA do to the brain?” (2006), http://www.drugabuse.gov/publications/mdma- ecstasy-abuse/what-does-mdma-do-to-brain.
5 Ralph Buchert et al., "Long-Term Effects of “Ecstasy” Use on Serotonin Transporters of the Brain Investigated by PET," Journal of Nuclear Medicine 44, no. 3 (2003): 375-84; Jennifer Do and Susan Schenk, "Self-administered MDMA produces dose- and time-dependent serotonin deficits in the rat brain," Addiction Biology 18, no. 3 (2013): 441-47.
6 AR Green et al., "Ecstasy cannot be assumed to be 3, 4‐ methylenedioxyamphetamine (MDMA)," British journal of pharmacology 166, no. 5 (2012): 1521-22.
7 See Ecstasydata.org, “Test Result Statistics: Summary Data,” (2015), http://www.ecstasydata.org/stats.php. See also, Tibor M Brunt et al., "Instability of the ecstasy market and a new kid on the block: mephedrone," Journal of Psychopharmacology 25, no. 11 (2011): 1543-47; E. E. Tanner-Smith, "Pharmacological content of tablets sold as "ecstasy": results from an online testing service," Drug Alcohol Depend 83, no. 3 (2006): 247-54; Neeltje Vogels et al., "Content of ecstasy in the Netherlands: 1993–2008," Addiction 104, no. 12 (2009): 2057-66; David Michael Wood et al., "Variability in the 3,4-methylenedioxymethamphetamine content of ‘ecstasy’ tablets in the UK," Emergency Medicine Journal 28, no. 9 (2011): 764-65.
8 Gina Martin et al., "Nonfatal overdose from alcohol and/or drugs among a sample of recreational drug users," Journal of Substance Use 19, no. 3 (2014): 239-44.
9 G. Rogers et al., "The harmful health effects of recreational ecstasy: a systematic review of observational evidence," Health Technol Assess 13, no. 6 (2009). See also, Emanuel Sferios and Missi Wooldridge, “MDMA-Related Deaths: Stop Calling Them Overdoses,” (July 10, 2015), https://dancesafe.org/mdma-related-deaths-stop-calling-them- overdoses/.
10 A. C. Parrott, "MDMA (3,4- Methylenedioxymethamphetamine) or ecstasy: the neuropsychobiological implications of taking it at dances and raves," Neuropsychobiology 50, no. 4 (2004); A. C. Parrott, "MDMA and temperature: a review of the thermal effects of 'Ecstasy' in humans," Drug Alcohol Depend 121, no. 1-2 (2012); K. Wolff and K. Aitchison, "Reply to 'MDMA can increase cortical levels by 800% in dance clubbers' Parrott et al," J Psychopharmacol 27, no. 1 (2013).
11 G. D. van Dijken et al., "High incidence of mild hyponatraemia in females using ecstasy at a rave party," Nephrol Dial Transplant 28, no. 9 (2013).
12 D. W. Lachenmeier and J. Rehm, "Comparative risk assessment of alcohol, tobacco, cannabis and other illicit drugs using the margin of exposure approach," Sci Rep 5(2015); J. van Amsterdam et al., "European rating of drug harms," J Psychopharmacol 29, no. 6 (2015).
13 David J Nutt, Leslie A King, and Lawrence D Phillips, "Drug harms in the UK: a multicriteria decision analysis," The Lancet 376, no. 9752 (2010): 1558-65.
14 See e.g., Jan van Amsterdam et al., "Ranking the harm of alcohol, tobacco and illicit drugs for the individual and the population," European Addiction Research 16, no. 4 (2010): 202-7.
15 Ecstasydata.org, “Test Result Statistics: Summary Data,” (2015), http://www.ecstasydata.org/stats.php.
16 David J Nutt, Leslie A King, and Lawrence D Phillips, "Drug Harms in the Uk: A Multicriteria Decision Analysis," The Lancet 376, no. 9752 (2010); David Nutt et al., "Development of a rational scale to assess the harm of drugs of potential misuse," The Lancet 369, no. 9566 (2007); van Amsterdam et al., "European rating of drug harms; Lachenmeier and Rehm, "Comparative risk assessment of alcohol, tobacco, cannabis and other illicit drugs using the margin of exposure approach."
17 See e.g., D. Wagner et al., "A prospective study of learning, memory, and executive function in new MDMA users," Addiction 108, no. 1 (2013): 136-45; T. Schilt et al., "Cognition in novice ecstasy users with minimal exposure to other drugs: A prospective cohort study," Archives of General Psychiatry 64, no. 6 (2007): 728-36.
18 S. de Sola et al., "Auditory event-related potentials (P3) and cognitive performance in recreational ecstasy polydrug users: evidence from a 12-month longitudinal study," Psychopharmacology (Berl) 200, no. 3 (2008): 425-37; R. Doblin et al., "A reconsideration and response to Parrott AC (2013) "Human psychobiology of MDMA or 'Ecstasy': an overview of 25 years of empirical research"," Hum Psychopharmacol 29, no. 2 (2014). Charles S Grob, "Deconstructing ecstasy: the politics of MDMA research," Addiction Research & Theory 8, no. 6 (2000): 549-88; A. R. Green et al., "Lost in translation: preclinical studies on 3,4- methylenedioxymethamphetamine provide information on mechanisms of action, but do not allow accurate prediction of adverse events in humans," Br J Pharmacol 166, no. 5 (2012).
19 John H. Halpern et al., "Residual neurocognitive features of long-term ecstasy users with minimal exposure to other drugs," Addiction 106, no. 4 (2011): 777-86. See also, J. H. Halpern et al., "Residual neuropsychological effects of illicit 3,4-methylenedioxymethamphetamine (MDMA) in individuals with minimal exposure to other drugs," Drug Alcohol Depend 75, no. 2 (2004): 135-47. G. Jager et al., "Incidental use of ecstasy: no evidence for harmful effects on cognitive brain function in a prospective fMRI study," Psychopharmacology (Berl) 193, no. 3 (2007): 403-14.
20 J. E. Fisk et al., "Modelling the adverse effects associated with ecstasy use," Addiction 106, no. 4 (2011): 798-85.
21 J. E. Fisk et al., "Temporal and visual source memory deficits among ecstasy/polydrug users," Hum Psychopharmacol 29, no. 2 (2014): 172-82; T. J. Watkins et al., "Human ecstasy (MDMA) polydrug users have altered brain activation during semantic processing," Psychopharmacology (Berl) 227, no. 1 (2013): 41-54.
22 Substance Abuse and Mental Health Services Administration, "Results from the 2013 National Survey on Drug Use and Health," (Rockville, MD: Substance Abuse and Mental Health Services Administration, 2014), Table 1.1B.
23 Ibid., Tables 7.5B & 7.6B.
24 Ibid., Tables 7.8B & 7.9B.
25 Lloyd D. Johnston et al., Monitoring the Future national survey results on drug use, 1975–2013: Volume 2, College students and adults ages 19–55 (Ann Arbor: Institute for Social Research, The University of Michigan, 2014), Table 2.3.
26 A. Winstock, "The Global Drug Survey 2014 findings," http://www.globaldrugsurvey.com/.
27 R. Doblin, “A clinical plan for MDMA (Ecstasy) in the treatment of posttraumatic stress disorder (PTSD): partnering with the FDA,” J. Psychoactive Drugs, 34 (2002):185-94.
28 Ben Sessa and David Nutt, "Making a medicine out of MDMA," The British Journal of Psychiatry 206, no. 1 (2015): 4-6.
29 Multidisciplinary Association of Psychedelic Studies, http://www.mdmaptsd.org.
30 M. C. Mithoefer et al., "The safety and efficacy of {+/-}3,4- methylenedioxymethamphetamine-assisted psychotherapy in subjects with chronic, treatment-resistant posttraumatic stress disorder: the first randomized controlled pilot study," J Psychopharmacol 25, no. 4 (2011).
31 P. Oehen et al., "A randomized, controlled pilot study of MDMA (+/- 3,4-Methylenedioxymethamphetamine)-assisted psychotherapy for treatment of resistant, chronic Post- Traumatic Stress Disorder (PTSD)," J Psychopharmacol 27, no. 1 (2013): 40-52; C. M. White, "3,4- Methylenedioxymethamphetamine's (MDMA's) Impact on Posttraumatic Stress Disorder," Ann Pharmacother 48, no. 7 (2014): 908-15; M. C. Mithoefer et al., "Durability of improvement in post-traumatic stress disorder symptoms and absence of harmful effects or drug dependency after 3,4- methylenedioxymethamphetamine-assisted psychotherapy: a prospective long-term follow-up study," J Psychopharmacol 27, no. 1 (2013): 28-39.
32 “A Randomized, Triple-Blind, Phase 2 Pilot Study Comparing 3 Different Doses of MDMA in Conjunction with Manualized Psychotherapy in 24 Veterans, Firefighters, and Police Officers with Chronic, Treatment-Resistant PTSD”, 2012, http://www.maps.org/research/mdma/MP8_amend4_final_7Feb2012w eb.pdf.